学术会议签到表
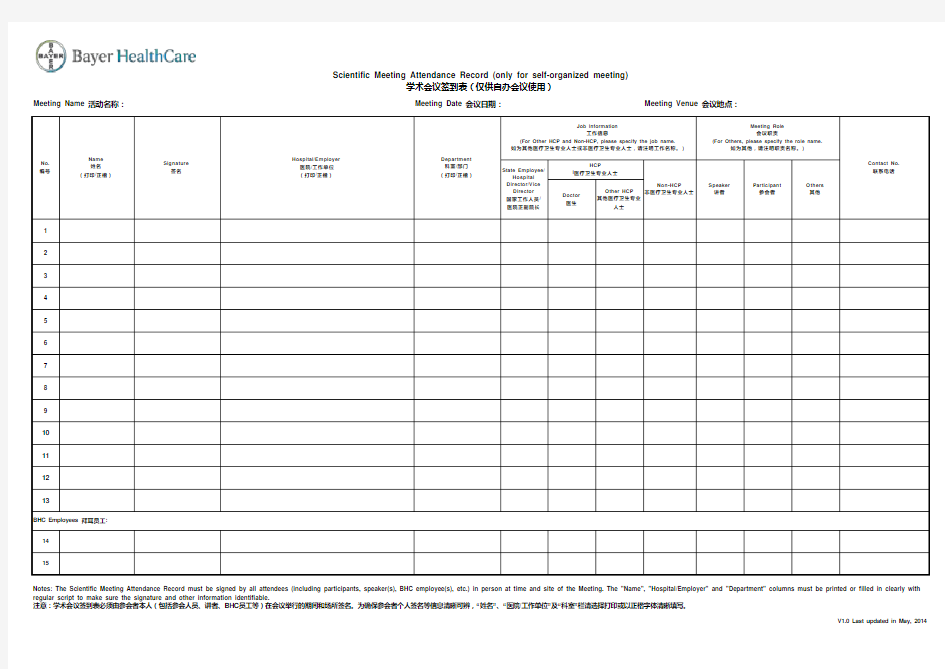
Meeting Name 活动名称:
Meeting Date 会议日期:
Meeting Venue 会议地点:
Doctor 医生
Other HCP 其他医疗卫生专业
人士
12345678910111213
14
15
Name 姓名
(打印/正楷)
Signature 签名
Hospital/Employer 医院/工作单位(打印/正楷)
Department 科室/部门(打印/正楷)
Participant 参会者
V1.0 Last updated in May, 2014
Scientific Meeting Attendance Record (only for self-organized meeting)
学术会议签到表(仅供自办会议使用)
BHC Employees 拜耳员工:Notes: The Scientific Meeting Attendance Record must be signed by all attendees (including participants, speaker(s), BHC employee(s), etc.) in person at time and site of the Meeting. The "Name", "Hospital/Employer" and "Department" columns must be printed or filled in clearly with regular script to make sure the signature and other information identifiable.
注意:学术会议签到表必须由参会者本人(包括参会人员、讲者、BHC 员工等)在会议举行的期间和场所签名。为确保参会者个人签名等信息清晰可辨,“姓名”、“医院/工作单位”及“科室”栏请选择打印或以正楷字体清晰填写。
Job Information
工作信息
(For Other HCP and Non-HCP, please specify the job name.如为其他医疗卫生专业人士或非医疗卫生专业人士,请注明工作名称。)
Meeting Role 会议职责
(For Others, please specify the role name.
如为其他,请注明职责名称。)
Contact No.联系电话
State Employee/
Hospital Director/Vice Director 国家工作人员/医院正副院长
HCP
l 医疗卫生专业人士
Non-HCP
非医疗卫生专业人士Speaker 讲者
Others 其他
No.编号